
When first I sit down with a new patient, I spend about 30 minutes talking to them.
Wait WHAT?!
Yes – I spend 30 whole minutes of time SPEAKING to them. LOOKING at them. And LISTENING. I have them tell their story about what brings them into my office, from the very beginning. I ask what they’ve tried that’s helped, what hasn’t, and I make them use that annoying 0-10 scale that everybody hates. But one of the most important things I’m doing during that conversation is I’m spying on them.
Let’s say that patient is coming in with complaints of neck pain. And the whole time he’s sitting there talking to me, he’s moving his head. He looks up when he’s thinking, he leans right when he’s listening, and when he REALLY gets worked up about how he’s feeling and how this has affected his life, he’s almost VIOLENTLY jutting his chin forward toward me for emphasis.

Yep that. I see that. All the time. It turns out that this patient gestures with his head, and moves excessively all day long. And that’s manifested as neck pain and headaches and it’s affecting his ability to work and do things like go out to dinner with friends and play his guitar.
So while you might think “Gee, some dry needles combined with Reiki on an inversion table” sounds like a solid plan here, I’m thinking:
“Get this guy to stop moving his head.”
I have a doctorate and that’s the BEST I CAN COME UP WITH?! Yes. It almost sounds too simple, right?
But the best solutions are elegantly simple. And the best solutions identify the root of the issue – in this gentleman’s case, cervical instability related to habitual and asymmetric movements that he does OVER AND OVER AND OVER. It stands to reason that if I do the dry needling with the Reiki on the inversion table and he goes home feeling really confident in me because I’m fancy, any relief he gets is going to last all of about 5 minutes because he’s going to keep moving his head too much and undo all my hard work. Or keep me in business because he’s going to be back the next week with the same symptoms.
Another example I see all the time:
A woman comes in the office with complaints of low back pain with walking. It’s limiting her ability to get exercise and manifesting in pain at nighttime and with bending and lifting. I watch her walk, and I’m struck by the amount of rotation happening at her hips when she moves her legs forward. It’s something like this:

I mean her walk has STYLE. If lumbar instability could be considered attractive.
So this time, I use a cupping technique followed by a blood flow restriction cuff while she strengthens with heavy weights.
Just kidding.
I teach her how to keep her hips still while she’s walking to reduce the microinstability at her lumbar spine.
Then I complement that with exercises that engage all the muscles that help keep her middle still while her extremities move. That’s called STABILIZATION, and it’s an essential part of any workout routine.
And if you’re wondering if I do any of the fun hands-on work, yes – I absolutely do. Partly because it can be a helpful to address tissue or joint restrictions that result from the movement issue, and also because it helps build trust. But it’s not the first place I go, and if it’s the first place your practitioner goes, you should be asking some questions.
So at that first visit, once I’ve done a thorough patient interview, physical and exam and identified some of these movement or positional “ingredients” for pain, I’ve taken to making all my patients listen to my lecture about what I call the “80/20 Rule”. Here’s what it is, and yes, I made the numbers up somewhat arbitrarily. But the basic premise – that identifying and eliminating faulty movement patterns and positions is MUCH more important to your outcome than any passive treatments or exercise you do – is well-supported by research.
Here’s what I hand to my patients:
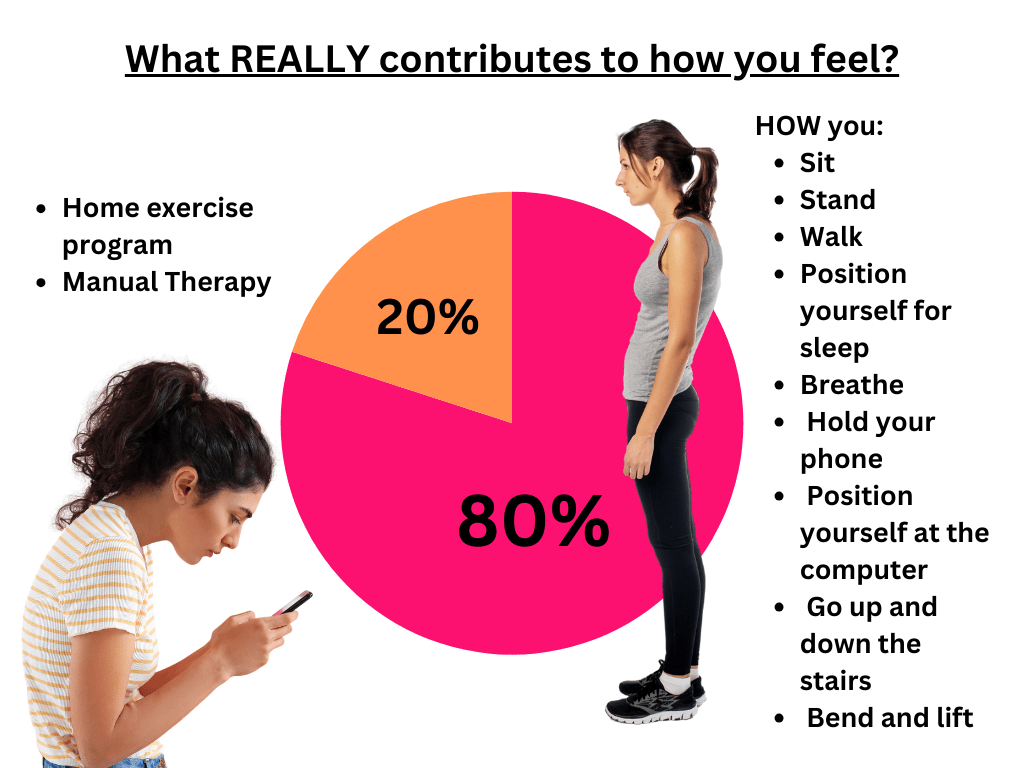
If you’ve gone through a whole bout of physical therapy care and you’re not where you need to be, consider that you haven’t been instructed on how to do things BETTER.
If your therapist saw something in your walking pattern that suggests hip weakness, did they just strengthen the hip, or did they also teach you how to walk better? Did you practice and have them watch you? And then re-check the next visit?
Because the presence of a muscle doesn’t dictate it’s function. Or – in other words – you can have a perfectly strong muscle that is out to lunch during function. You have to re-train the movement, not just the muscle. That’s how you feel better in the short-term AND the long-term.
So I ask again:

Leave a comment