Breathing is, well, kind of BASIC. If we don’t do it, we die. Obviously. But is it possible to breathe incorrectly? From an orthopedic perspective, absolutely YES. Just like our other movement patterns, from walking to turning over in bed, our breathing patterns can become very disordered, and that has serious implications.
As usual, let’s start from the beginning. The function of breath coming into and going out of our bodies is to bring in oxygen and to remove carbon dioxide. From a cellular perspective, we need the efficient movement of those vital gases to sustain life. From a musculoskeletal perspective, though, there is another important function, and that is to regulate the amount of pressure in the core. Let’s think of the core like a canister:

The walls of the canister are made up of the abdominal wall – 4 wonderful layers of muscle that hold in the vital organs and support the spine. The bottom of the canister is the pelvic floor (think kegels) and the top is the diaphragm. WHAT?! The diaphragm is part of the core? It sure is. When’s the last time you knowingly used it?
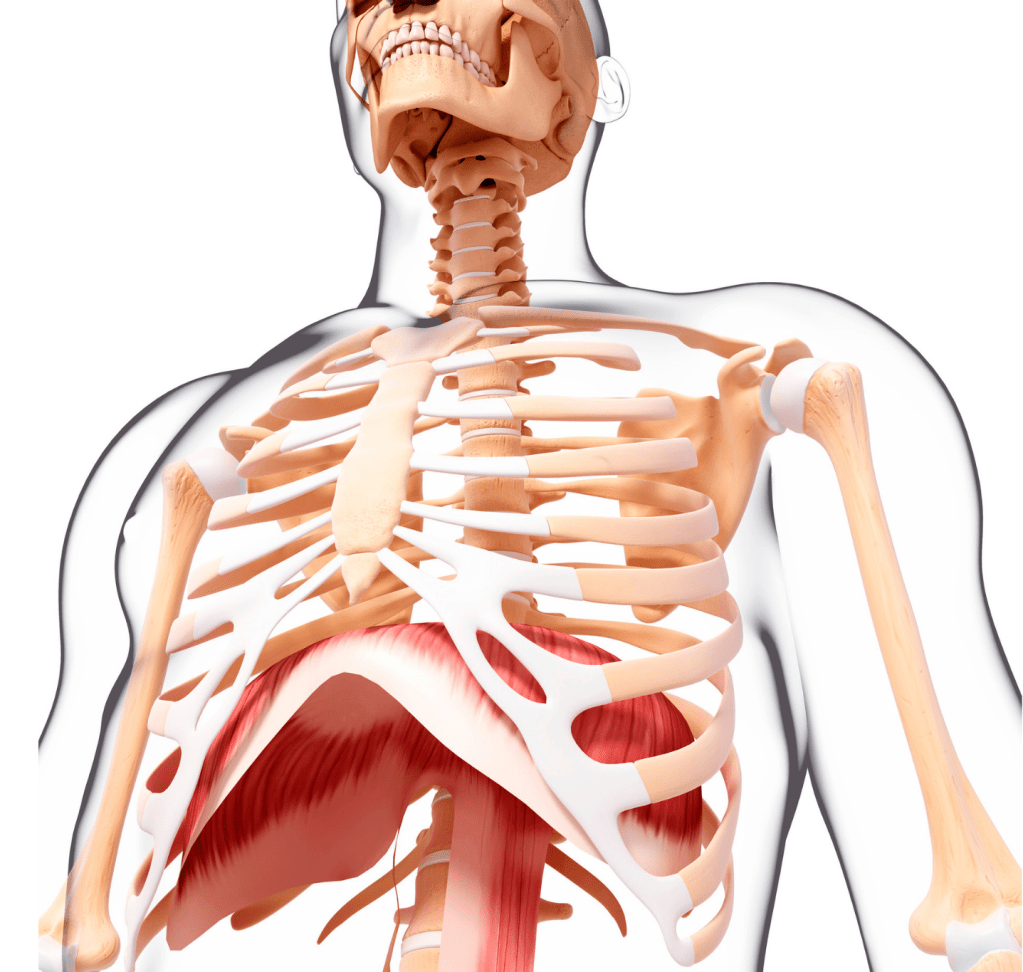
The diaphragm is a dome-shaped muscle that is key to the process of breathing. When we inhale, the diaphragm pushes down, increasing the amount of pressure in the abdominal cavity and sucking air into the lungs. When we exhale it rises up under our lungs, thereby decreasing pressure in the abdomen. What does an increase or decrease in pressure in the abdomen regulate? Stability in the spine, for one thing.
You’ve probably heard the term “diaphragmatic breathing”. What that term means, in a nutshell, is that when you inhale your breath has a certain order of operations. If you’re breathing diaphragmatically, which is the most efficient way to move gases and regulate your abdominal pressure, your belly inflates with an inhale and deflates with an exhale. In a relaxed state (not exercising), your tongue is in the roof of your mouth, you primarily breathe through your nose and the belly inflates first, followed by the lower ribs, followed by the upper ribs. Rinse and repeat. Try this: put one hand on your belly and one hand on your ribs. As you inhale gently, try to make your belly hand rise first.

What if, though, instead of letting your belly gently inflate, you’ve arrived at the habit of holding your belly in like you’ve just eaten a big Thanksgiving dinner and you’re walking down the beach with your shirt off? Maybe you started doing this because, literally, you just ate a big Thanksgiving dinner and you’re walking down the beach with your shirt off. Or maybe, somewhere along the line, someone – perhaps a well-intentioned personal trainer or PHYSICAL THERAPIST – told you that was the way to activate your core. And you trusted them. You did the exercise where you pull your belly button in and hold it. Over and over and over. And then, naturally, you translated that over to function. It made your back feel a little better, so you started holding your belly button in when you were standing making dinner, and taking a walk with your wife, and even sitting at your desk during the day. Fast forward 20 years: your back is still on edge. You can keep it under the radar if you have your gut sucked in all the time, but periodically it “goes out” and you’re debilitated for several days. That’s just life past 40, right? Meanwhile you’ve started to notice that your lower ribs stick out WAY more than they used to – what’s with that?!

If you’re not in the tummy holding vanity category, but were actually trained by a health professional to hold your belly in, here’s why. There is a muscle, actually the deepest abdominal layer, called the transversus abdominis. Its function is to squeeze your middle like a corset, decompressing your spinal segments – basically opposing the force of gravity. It gives your back tremendous resilience against outside forces, which is wonderful. Support for everything from lifting a box to shoveling your driveway! What happened is that sometime in the not too distant past, EMG studies were done that showed that, during an acute episode of back pain, the transversus leaves you high and dry. It’s like:

Thanks transversus. It stops decompressing you, and as a result the previous resilience to outside forces you enjoyed is a thing of the past. What’s more, it doesn’t seem that the transversus decides to start working normally again following an episode of back pain. It either decides to come on late during a task or – even worse – not at all.
So the solution to this, at least in my field, was to take the fact that the transversus shuts down and

We blew it up to such epic proportions that we started training people to walk around with an activated abdominal corset all day long. An over-reaction? I’d say so, but you’ll still find many people that disagree with me. The transversus is not a muscle that was meant to be “on” all day long. Just like any muscle, it should have some stiffness – you don’t want a saggy baggy transversus. And it should turn on in anticipation of an outside force. My brain says “I’m going to pick up this boulder”. The transversus turns on a fraction of a second early in preparation and I lift that boulder like it was a pebble. Wonderful! What a fabulous muscle. But what happens if the transversus, instead of being used in an activity-dependent, intermittent fashion – becomes a muscle that’s pretty much on all the time?
The answer is that it obliterates the appropriate use of the diaphragm, the top of our core canister. Instead of inflating the belly on the inhale, we don’t inflate the belly but we instead over-inflate the lower ribs to get in enough air. Do that over and over all day, all night for years and your lower ribs start to reach for your chin. And given that the lower ribs are the upper attachment point of the abdominal wall, what do you think that does to the length-tension relationship of the abdominal wall? Not great things. You now have an impressively over-active transversus and a practically paralyzed diaphragm. No wonder your back is on a hair trigger! By the way, if you don’t know what I’m talking about when I say “length-tension relationship”, go back and read my previous post: SET YOUR MUSCLES UP FOR SUCCESS: defining the length-tension relationship.
So what is the correct way to use your core, and should it literally be “on” all day long? I believe the correct answer to this question lies, first and foremost, in aligning the body the way it was meant to be aligned so that the length-tension relationships of the core muscles are ideal. I teach my patients what it feels like in various positions to have the rib cage (thorax) and the pelvis both vertical and the plumbline from the shoulder falling perfectly to hip:

THEN, I teach breathing pattern in those positions, starting from lying down with the knees bent because that’s always the easiest place to start. For some people, this means a little pelvic tilt. For others, it means bringing the lower ribs down (try laughing – you’ll see what that feels like). For many, it’s a little bit of both. We get the thorax and the pelvis vertically aligned with one another and then we practice breathing diaphragmatically while holding the position. It’s deeply calm – not “activated”. THEN, once the patient knows how to hold the spine in neutral with diaphragmatic breathing, we start to add very simple movement – a march of the knee or a tilt of the thigh – making sure the pelvis and the rib cage stay still (stable) and breathing remains diaphragmatic. What do you think happens when you get yourself aligned, inhale diaphragmatically and then, on the exhale, lift a knee? Well the ribs descend and the transversus turns on, so that’s wonderful. Then you lower your knee and it turns off – equally wonderful. And you’ve taught yourself a method of movement that preserves the balance of pressure in the abdominal cavity and, thus, the stability in the spinal column. NOW rinse and repeat.